





Appointments
Request Appointment/Request Exam - After completing the respective forms, these requests will be processed by our services, and you will receive confirmation by email. The indications about the Agreements (Insurance/Subsystem) are merely informative, please request confirmation in the "Observations" field.
Schedule Appointment/Exam myHPA - By accessing myHPA Saúde you can make the appointment in real time, directly on the Doctor's schedule according to his availability.
You can also contact us at +351 282 420 400 Algarve | +351 269 630 370 Alentejo | +351 291 003 300 Madeira
(National landline)
Your request has been successfully received. We will confirm your appointment shortly.
Download myHPA Saúde:


HPA Health Group Newsletter:
Subscribe and stay up to date with all the news!
Dr. Duarte Freitas
Radiologista

Steatosis / Steatohepatitis:
The good, the bad and the villain
HPA Magazine 15
Liver steatosis/steatohepatitis, commonly known as fatty liver, is the most prevalent chronic liver disease in Western societies. The prevalence in the general population is estimated to be around 30%.
It is the most frequent cause of liver disease, altered blood analysis, and a frequent cause for imaging scans.
Although steatohepatitis is found in patients with a high alcohol consumption, non-alcoholic cases are increasingly common.
There are two non-alcoholic fatty liver phenotypes: (NAFLD: non-alcoholic fatty liver disease) and (NASH: non-alcoholic steatohepatitis).
Fatty liver refers to the accumulation of triglycerides in the cells of the liver: hepatocytes. Histological diagnosis is made by means of a liver biopsy and graded from 0 (<5% hepatocytes containing fat vacuoles), grade 1 (5-33%), grade 2 (33-66%), grade 3 (> 66%).
The key histological difference between NAFLD and NASH is the presence of inflammation in NASH; it is the inflammation that will potentially cause liver damage and is defined by the presence of inflammatory cells in liver biopsies.
While simple steatosis (NAFLD) is relatively benign, steatohepatitis (NASH) has the potential to progress to liver cirrhosis.
Liver cirrhosis occurs when there is fibrosis in the liver with disorganization of its structure and, more importantly, its function. Complications of cirrhosis include encephalopathy, ascites, and potentially hepatocarcinoma.
CAUSES
When fatty liver is mentioned, the first association is the consumption of alcohol. This is a recognized cause of steatosis and particularly steatohepatitis.
However, it is not the only one; 80% of obese people surfer with NAFLD. It is also potentially the most recoverable cause of the disease. A calorie-restriction diet combined with physical exercise has a profound impact on the improvement and progression of the disease, particularly because obesity is often associated with high blood pressure, diabetes and dyslipidemia.
Cardiovascular risk also increases and is the leading cause of death in people with NAFLD.
The progression from NAFLD to NASH occurs in 6-26% of patients, resulting in increased morbidity and mortality due to cirrhosis and its complications.
So as not to become exhaustive in discussing all causes of fatty liver, other causes such as hepatitis C, metabolic diseases, glycogen storage diseases, toxic and side effects of medication has not been discussed.
DIAGNOSIS
Probably, the first indication that the patient suffers from fatty liver, are results of clinical analyses due to high levels of liver enzymes ALT and AST. Further diagnostic scans are often needed. Several diagnostic imaging scans can be performed:
Ultrasound
The diagnosis accuracy of ultrasound for detection of fatty liver varies between 80 and 89%.
The radiologist tries to detect the increased brightness of the liver, a marker for steatosis.
As the steatosis worsens, the opposite phenomenon occurs, the brightness decreases, in extreme cases, the liver is so obscure that it becomes inaccessible to ultrasound evaluation.
In addition to searching steatosis, signs of more advanced liver disease is also sought. In cases of cirrhosis, elastography is available, which can also detect fibrosis of the liver.
CT SCAN – Computed Tomography Scan
CT Scan is not the first-line test for diagnosing fatty liver, not because it is not a capable method, but because it involves radiation, and as such, it is not the best screening test. However, it will be a good option if the doctor suspects a more serious illness or complications.
MRI – Magnetic Resonance Imaging
An MRI scan is the best imaging method to diagnose liver disease. Like the CT Scan, it is a complex scan, not ideal as a screening method, but used to obtain a specific diagnosis. The results obtained with MRI scans are superior to other imaging modalities as it is possible to obtain excellent tissue characterization. When compared to CT Scans, it has the advantage of not having X-ray radiation. It is the preferred method for assessing the liver in young people, where the organs are more radiosensitive.
Using appropriate sequences, it is possible to quantify the intracellular fat of hepatocytes (Fig. 7).
TREATMENT
The treatment of fatty liver lies in treating the underlying cause. In the initial stage it is reversible. By suspending the consumption of alcohol, together with a diet plan provided by the nutritionist, controlling diabetes, dyslipidemia and high blood pressure.
The evolution of a fatty liver into cirrhosis will require treatment of its complications and, ultimately, a liver transplant.
CONCLUSION
We began this article with the good, the bad (steatosis) and the villain (steatohepatitis). But the good has not yet materialized.
However, the good has been mentioned throughout this article and it is now time to reveal its identity.
It is science, that provides all the necessary data and evidence, they are the health professionals who treat the patients and also the methods of diagnosis that permit us to treat diseases and change their natural course and, above all, the willpower of each one of us, in implementing lifestyle changes to our daily lives.
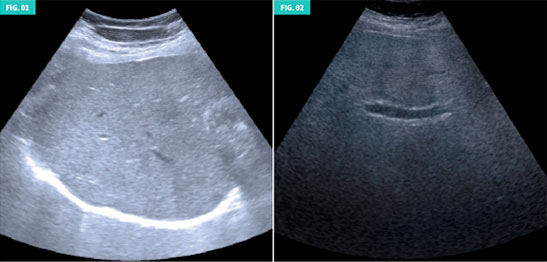
Figure 1 (left): Low-grade hepatic steatosis.
Figure 2 (right): High-grade hepatic steatosis.Note that with the exception of the Portal vein, (centre of the image) few details of the liver's structure are discernable.
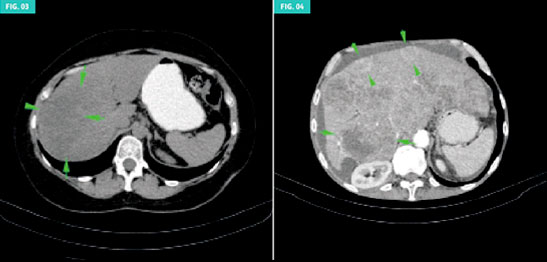
Figure 3 (left): A liver mass was suspected in the right lobe of this patient, with hepatomegaly and steatosis. However, after contrast administration, it was found to be a focal pattern of steatosis, not a hepatocarcinoma.
Figure 4 (right): In this patient, with an enlarged liver, several hepatic nodules were detected that enhance contrast in the arterial phase, highly suggestive of hepatocellular carcinoma. In addition to the liver lesions, there is also ascites in the upper abdomen.

Figure 5 (left): Out-of-phase T1 sequence: In this patient, several hepatic nodules were suspected, but in this sequence, the outline of the nodules is accentuated, reflecting a diagnosis of nodular steatosis, a rare variant of steatosis.
Figure 6 (right): Out-of-phase T1 sequence: This patient with a steatosic pattern, shows signs of liver cirrhosis, with hepatomegaly and nodular contours.


Figure 7: Graphic result of specific sequences for the detection of steatosis. It permits the percentage quantification of hepatocytes with fat vacuoles. In this case the result was 12-18%.